
There is no official awareness ribbon color for adrenocortical carcinoma(ACC), definitely not one that would be recognizable since it is such a rare cancer. This is not a cancer that is seen very often in the general population, but it is one of the core LFS tumors. Adrenal tumors linked to LFS usually happen in early childhood, but can be seen at any age. As tumors grow on the adrenal gland, hormone production can increase and symptoms might be similar to those of puberty- increased hair growth, weight gain, and change in genitals- all this can happen in children who are much too young to even be in school yet. About 80% of pediatric ACC cases are caused by a p53 mutation but less than 10% of people with LFS will actually be diagnosed with ACC. These numbers show that ACC is rare, even in LFS but that most cases of pediatric ACC can be linked to LFS.
Adrenocortical carcinoma in children in the general population is even more rare- less than 1 case per million people. Yet in southern Brazil, there are 10-15 times as many cases of pediatric ACC than in the general population. In the late 1980's Dr. Raul Ribeiro finished his fellowship at St. Jude's Research Hospital and returned home to Brazil. He noticed a high incidence of rare ACC in the children there. Dr. Ribeiro suspected that these children had LFS due to the prevalence of ACC and it's association with the family cancer syndrome. When he did family histories, there was no higher incidence of any other typical LFS cancers. After genetic testing, they found the children did not have a typical p53 germline mutation. Scientists were stumped and decided to go looking outside of the DNA area that is usually mutated in LFS. There they found the unique mutation associated with the Brazilian ACC at another p53 locus called R337H. The full story can be read here.
The R337H mutation, although not the typical LFS mutation is LFS-like. It gives insight into a specific region on DNA. When that region is mutated, ACC develops. In Brazil, a screening program is in place to try and find those susceptible to this disease and treat it at the most curable stages. There is also research into possible environmental causes and other links. Dr. Ribeiro and his colleagues started a tumor registry to collate all pediatric adrenal tumor data internationally, called IPACTR. It is the first database of its kind and is a way of collecting tumor samples and information that will hopefully lead to more knowledge on the tumors, better treatments, and prevention.

Dr. Ribeiro at St. Jude's has been a champion for the smallest ACC sufferers. He has vast knowledge and experience with pediatric ACC and spends part of his time fielding calls from parents and helping them through their child's ACC diagnosis. He is one of the rare doctors, exemplifying how the relationship between patient and clinical research can be imperative in better treatments. His team is largely responsible for the pediatric clinical trial for ACC treatment with Mitotane.
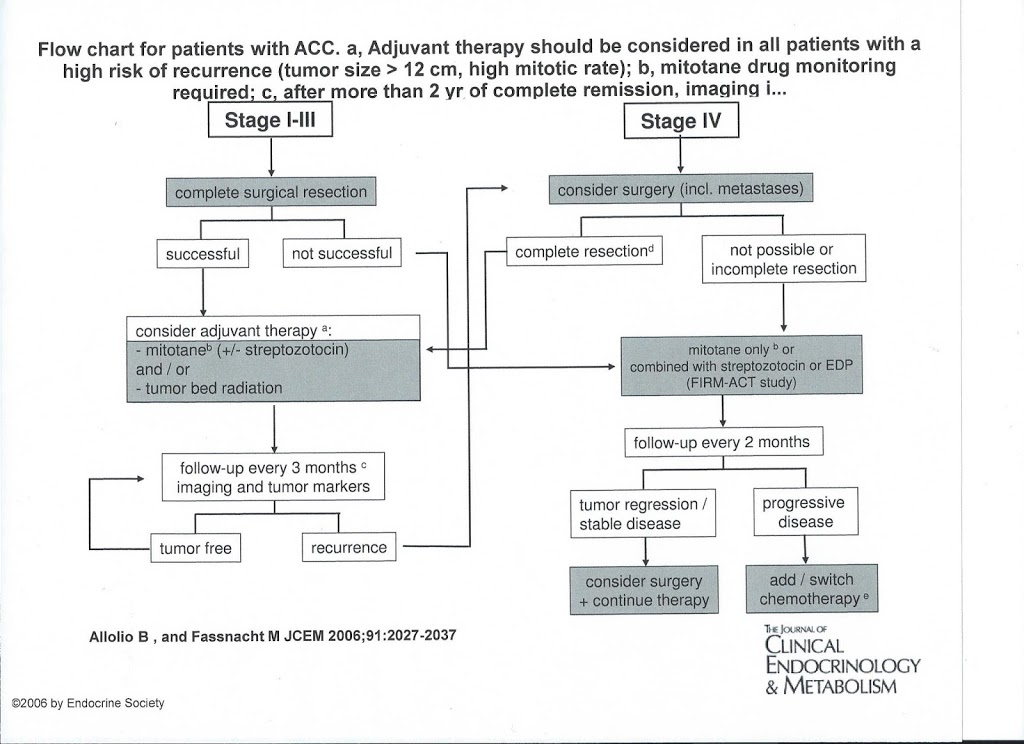
Surgical removal of all tumor is the best chance for curing pediatric ACC. Especially in LFS, ACC tends to be fairly aggressive and can come back or metastasize. In cases where the tumor is very large or there might be tumor cells remaining after surgery, chemotherapy will usually be recommended. Standard chemotherapeutic agents such as Doxorubicin, Etoposide and Cisplatin might be used along with(adjuvant) an adrenal specific drug called Mitotane. Mitotane is a relative of DDT- the pesticide years ago that Rachel Carson wrote about in the book Silent Spring. When the DDD isomer(slightly different chemical version) was used, researchers noticed that it caused adrenal suppression in dogs. Although normally, adrenal gland suppression is bad- this activity is beneficial in stopping out of control adrenal cancer cells. The drug Mitotane was tested and used to treat overactive adrenals in animals and is currently being studied for effectiveness in treating pediatric ACC. Information on the Children's Oncology Group Phase 3 Clinical Trial can be found here.
Due to it's rarity- like LFS- there is no official screening regimen for ACC in the general population. Although a diagnosis of ACC in a child should be a flag to doctors of a potential hereditary mutation(not just LFS) and genetic counseling and testing should be recommended, regardless of family history of cancer. The Toronto Protocol for LFS does however address the need for screening this cancer in children with p53 mutations. Fortunately there are specific endocrine labs that will catch excessive hormones caused by adrenal tumors and they can also be visible by ultrasound, MRI or CT. As a parent, it can be scary to think about all of the cancers your child might get. When you have LFS, it is important to know a bit about each cancer and know what symptoms to look for. Sometimes there are no symptoms with adrenocortical carcinoma. But any time you are concerned that your child might be developing too soon or exhibits symptoms of puberty in early childhood- it is important to be aware of this core tumor and have them checked by a physician. Great strides are being made by St. Jude's and other researchers to detect and cure Adrenocortical Carcinoma, especially in families with LFS.
References
IPACTR- St. Jude's International Pediatric Adrenocortical Tumor Registry


